Volume 110, Nº 5, May 2018
DOI: http://www.dx.doi.org/10.5935/abc.20180071
ORIGINAL ARTICLE
Pulmonary Vein Anatomy is Associated with Cryo Kinetics during Cryoballoon Ablation for Atrial Fibrillation
Xiongbiao Chen
Pihua Fang
Zheng Liu
Jia He
Min Tang
Jun Liu
Bin Lu
Shu Zhang
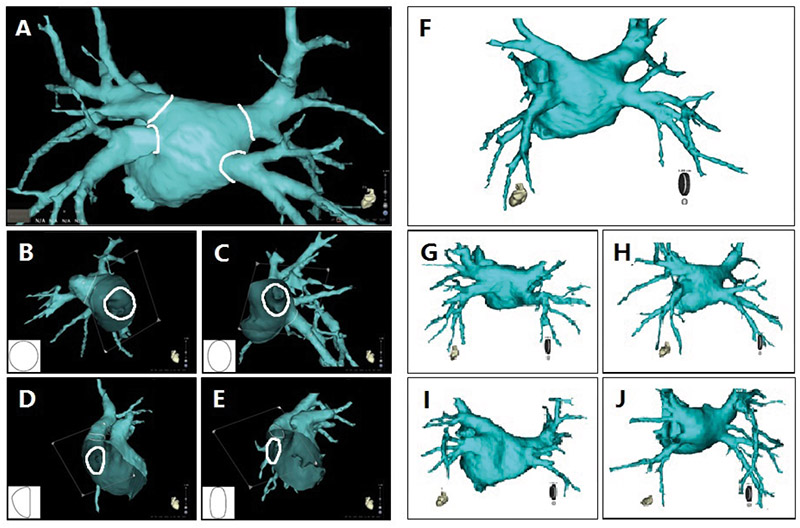
Figure 1 – PV ostium shapes category and PV drainage patterns. A) PV ostia depicted semi-automatically using CartoMerge software. Four shapes of PV ostium; B) Type I (round); C) Type II (oval); D) Type III (triangular); and E) Type IV (narrow). Five patterns of PV drainage; F) Four PVs drains into LA in a typical pattern; G) Left superior and inferior PVs drains into LA both in a pattern of with common trunk; H) Left superior and inferior PVs drains into LA both in a pattern of with common antrum; I) Right inferior PV drains into LA in a pattern of with ostial branch; J) Right superior and inferior PVs drains in LA with supernumerary vein (middle vein).
Abstract
Background: The influence of pulmonary vein (PV) anatomy on cryo kinetics during cryoballoon (CB) ablation is unclear.
Objective: To investigate the relationship between PV anatomy and cryo kinetics during CB ablation for atrial fibrillation (AF).
Methods: Sixty consecutive patients were enrolled. PV anatomy, including ostial diameters (long, short and corrected), ratio between short and long diameters, ostium shape (round, oval, triangular, and narrow), and drainage pattern (typical, with common trunk, common antrum, ostial branch and supernumerary PV) were evaluated on multi-detector computed tomography (MDCT) images pre-procedure. Cryo kinetics parameters [balloon freeze time from 0 to -30°C (BFT), balloon nadir temperature (BNT) and balloon warming time from -30 to +15°C (BWT)] were recorded during procedure. All p values are two-sided, with values of p < 0.05 considered to be statistically significant.
Results: 606 times of freezing cycle were accomplished. Moderate negative correlation was documented between BNT and corrected PV diameter (r = -0.51, p < 0.001) when using 23-mm CBs, and mild negative correlation (r = - 0.32, p = 0.001) was found when using 28-mm CBs. Multivariate logistic regression analysis revealed that PV corrected ostial diameter (OR, 1.4; p = 0.004) predicted a BNT < -51°C when using 23-mm CBs, while PV ostium oval shape (OR, 0.3; p = 0.033) and PV locations (left inferior PV: OR, 0.04; p = 0.005; right superior PV: OR, 4.3; p = 0.025) predicted BNT < -51°C when using 28-mm CBs.
Conclusions: MDCT can provide PV anatomy accurate evaluation prior CB ablation. PV anatomy is associated with cryo kinetics during ablation. (Arq Bras Cardiol. 2018; 110(5):440-448)
Keywords: Pulmonary Veins / anatomy & histology; Atrial Fibrillation; Catheter Ablation; Multidetector Computed Tomography; Cost-Benefit Analysis.