Volume 115, Nº 2, August 2020
DOI: https://doi.org/10.36660/abc.20190267
ORIGINAL ARTICLE
Custodiol®-HTK Solution vs. Cold Blood Cardioplegia for Isolated Coronary Surgery Requiring Prolonged Cross-Clamp Time: A Propensity-Matched Analysis
Giuseppe Gatti
Pierpaolo Taffarello
Gabriella Forti
Carla Gripari
Gianfranco Gustin
Gianluca Castaldi
Ilaria Fiorica
Aniello Pappalardo
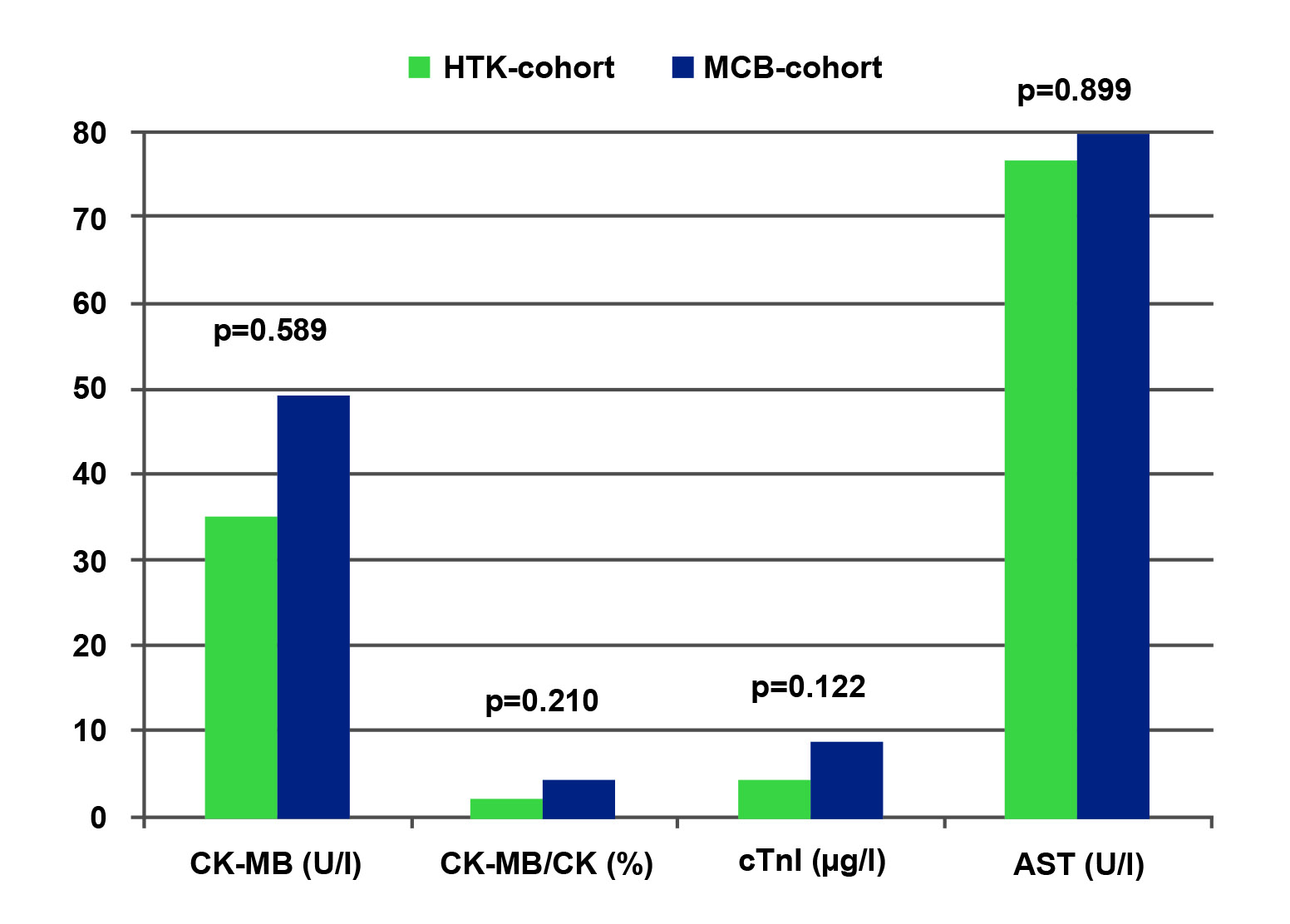
Figure 2 – HTK vs. MCB cohort. PS-matched pairs. Differences on peak serum levels after surgery of CK-MB, CK-MB/CK, cTnI and AST. AST: aspartate aminotransferase; CK: creatine kinase; CK-MB: creatine kinase-MB; cTnI: cardiac troponin I; HTK: histidine-tryptophan-ketoglutarate; MCB: multidose cold blood; PS: propensity score.
Abstract
Background: Custodiol®-histidine-tryptophan-ketoglutarate (HTK) cardioplegia is widely used.
Objective: To compare the outcomes of isolated coronary surgery requiring prolonged cross-clamp time (XCT) in patients receiving a single-dose HTK or multidose cold blood (MCB) cardioplegia.
Methods: XCT was ≥120 minutes for 148 consecutive patients undergoing isolated coronary surgery (2009−2016). HTK and MCB cardioplegia were used in 38 and 110 cases, respectively. The two cohorts were compared on baseline characteristics, operative data, and early outcomes. Because risk profile and operative data differed significantly between the two groups, one-to-one propensity score-matched analysis was performed and 34 pairs were generated.
Results: While expected operative risk was higher in the HTK than in the MCB cohort (European System for Cardiac Operative Risk Evaluation II, p=0.005), there was no significant intergroup difference regarding in-hospital mortality (p=0.573). Overall (positive) postoperative fluid balance (p=0.003), number of blood transfusions (p=0.017), rates of acute kidney injury (p=0.002) and any major complication (p=0.019) were increased in HTK patients. These results were all confirmed even after propensity matching, though the difference was significant only for fluid balance (p=0.013) and quite significant for blood transfusions (p=0.054). In the HTK cohort, intensive care unit and hospital stay were longer both for overall (p=0.016 and 0.008) and matched patients (p=0.142 and 0.198). In matched patients, peak sérum levels of cardiac troponin I were lower in the HTK cohort (p=0.122); serum levels of creatinine were lower in the MCB cohort (p=0.023).
Conclusion: For the patients of this study who required prolonged XCT, there was a trend towards poorer outcomes when HTK, rather than MCB cardioplegia, was used. (Arq Bras Cardiol. 2020; 115(2):241-250)
Keywords: Myocardial Revascularization/complications; Heart Arrest Induced; Cardioplegic Solutions/thertapeutic use; Myocardial Reperfusion; Postoperative complications; Myocardial Infarction, Stroke; Mortality.