Volume 112, Nº 6, June 2019
DOI: http://www.dx.doi.org/10.5935/abc.20190027
ORIGINAL ARTICLE
Behavioral Influence of Known Prognostic Markers on the Cardiologist’s Decision following Acute Coronary Syndrome: the GRACE Score Paradox
Manuela Campelo Carvalhal
Thiago Menezes Barbosa de Souza
Jessica Suerdieck
Fernanda Lopes
Vitor Calixto de Almeida Correia
Yasmin Falcon Lacerda
Nicole de Sá
Gabriella Sant'Anna Sodré
Marcia Maria Noya Rabelo
Luis Cláudio Lemos Correia
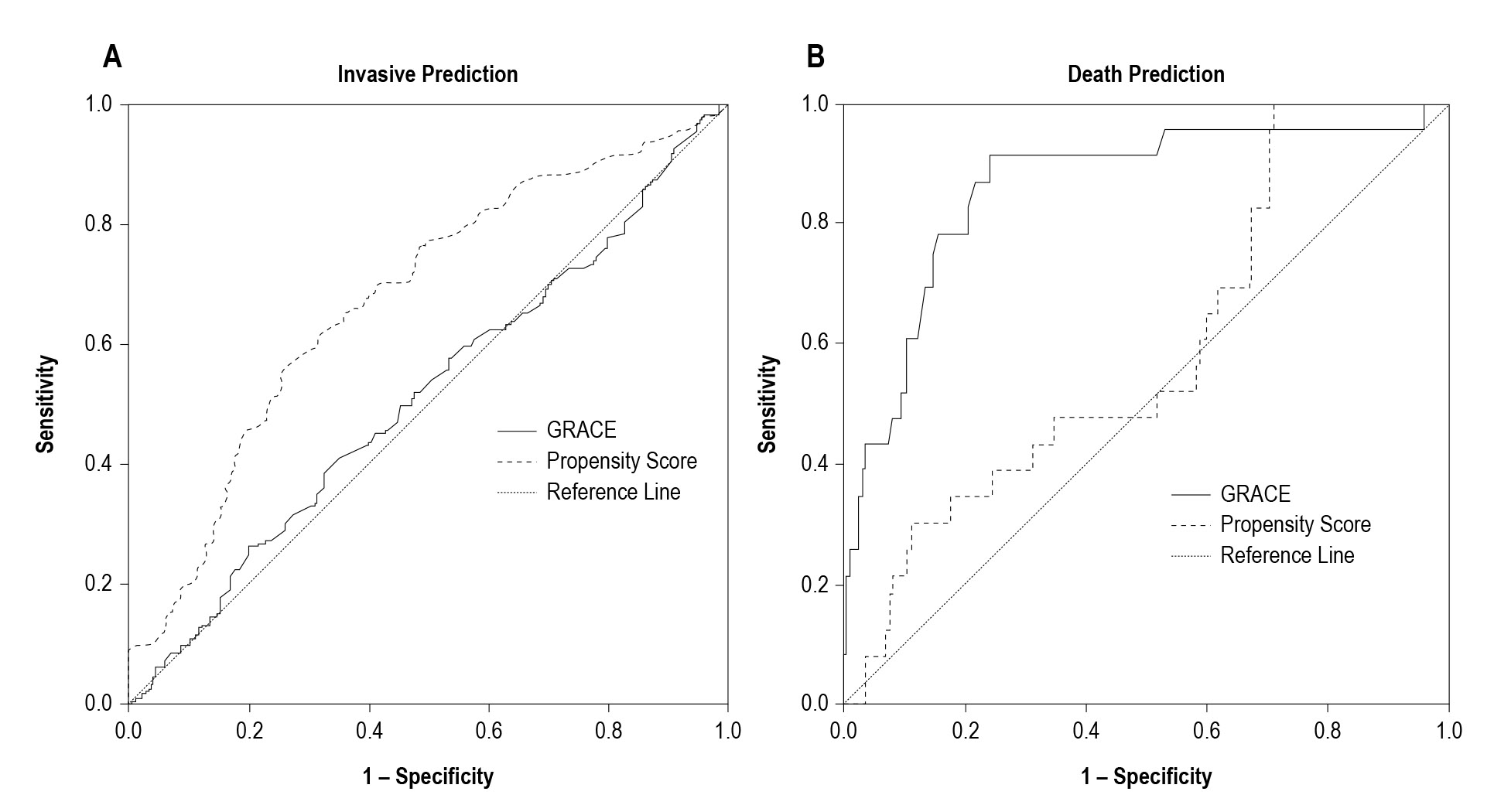
Figure 1 – According to the area under the curve, GRACE Score does not predict an invasive strategy, as opposed to the propensity score (Panel A, p < 0.001 for curve comparison). Conversely, GRACE Score is better than the propensity Score for the prediction of mortality (Panel B, p < 0.001).
Abstract
Background: Behavioral scientists consistently point out that knowledge does not influence decisions as expected. GRACE Score is a well validated risk model for predicting death of patients with acute coronary syndromes (ACS). However, whether prognostic assessment by this Score modulates medical decision is not known.
Objective: To test the hypothesis that the use of a validated risk score rationalizes the choice of invasive strategies for higher risk patients with non-ST-elevation ACS.
Methods: ACS patients were consecutively included in this prospective registry. GRACE Score was routinely used by cardiologists as the prognostic risk model. An invasive strategy was defined as an immediate decision of the coronary angiography, which in the selective strategy was only indicated in case of positive non-invasive test or unstable course. Firstly, we evaluated the association between GRACE and invasiviness; secondly, in order to find out the actual determinants of the invasive strategy, we built a propensity model for invasive decision. For this analysis, a p-value < 0.05 was considered as significant.
Results: In a sample of 570 patients, an invasive strategy was adopted for 394 (69%). GRACE Score was 118 ± 38 for the invasive group, similar to 116 ± 38 for the selective group (p = 0.64). A propensity score for the invasive strategy was derived from logistic regression: positive troponin and ST-deviation (positive associations) and hemoglobin (negative association). This score predicted an invasive strategy with c-statistics of 0.68 (95%CI: 0.63-0.73), opposed to GRACE Score (AUC 0.51; 95%CI: 0.47-0.57).
Conclusion: The dissociation between GRACE Score and invasive decision in ACS suggests that the knowledge of prognostic probabilities might not determine medical decision. (Arq Bras Cardiol. 2019; 112(6):721-726)