Volume 111, Nº 4, October 2018
DOI: http://www.dx.doi.org/10.5935/abc.20180159
ORIGINAL ARTICLE
Relationship of Electromechanical Dyssynchrony in Patients Submitted to CRT With LV Lead Implantation Guided by Gated Myocardial Perfusion Spect
Erivelton Alessandro do Nascimento
Christiane Cigagna Wiefels Reis
Fernanda Baptista Ribeiro
Christiane Rodrigues Alves
Eduardo Nani Silva
Mario Luiz Ribeiro
Claudio Tinoco Mesquita
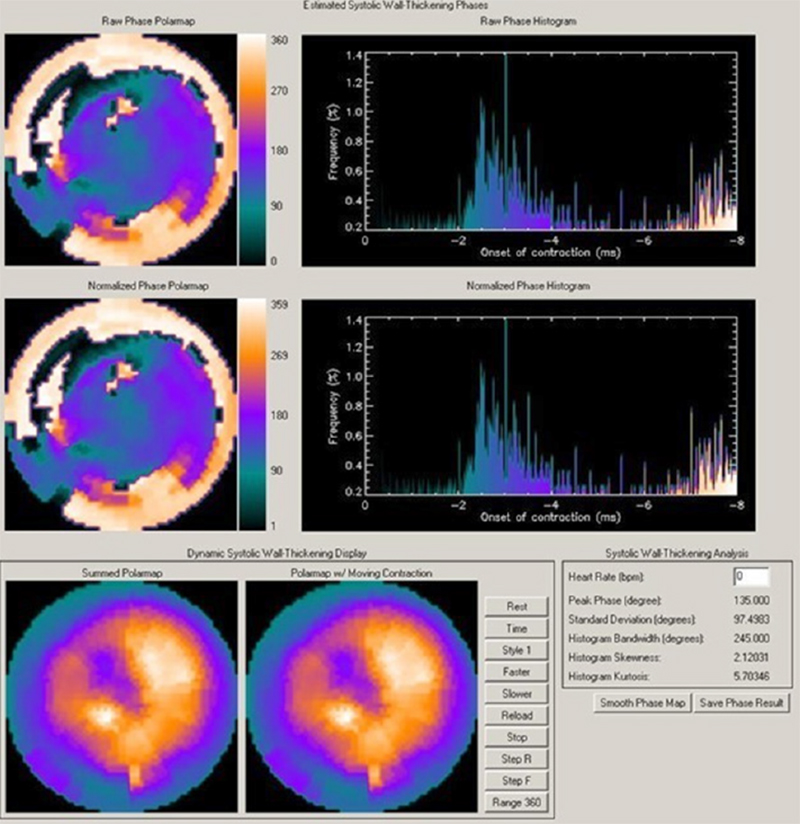
Figure 2 – Gated myocardial perfusion SPECT with analysis of ventricular synchronism in a patient with dilated cardiomyopathy and left bundle-branch block, showing marked dyssynchrony with HBW of 245° and SD of 97°.
Abstract
Background: Heart failure (HF) affects more than 5 million individuals in the United States, with more than 1 million hospital admissions per year. Cardiac resynchronization therapy (CRT) can benefit patients with advanced HF and prolonged QRS. A significant percentage of patients, however, does not respond to CRT. Electrical dyssynchrony isolated might not be a good predictor of response, and the last left ventricular (LV) segment to contract can influence the response.
Objectives: To assess electromechanical dyssynchrony in CRT with LV lead implantation guided by GATED SPECT.
Methods: This study included 15 patients with functional class II-IV HF and clinically optimized, ejection fraction of 35%, sinus rhythm, left bundle branch block, and QRS ≥ 120 ms. The patients underwent electrocardiography, answered the Minnesota Living with Heart Failure Questionnaire (MLHFQ), and underwent gated myocardial perfusion SPECT up to 4 weeks before CRT, being reassessed 6 months later. The primary analysis aimed at determining the proportion of patients with a reduction in QRS duration and favorable response to CRT, depending on concordance of the LV lead position, using chi-square test. The pre- and post-CRT variables were analyzed by use of Student t test, adopting the significance level of 5%.
Results: We implanted 15 CRT devices, and 2 patients died during follow-up. The durations of the QRS (212 ms vs 136 ms) and the PR interval (179 ms vs 126 ms) were significantly reduced (p < 0.001). In 54% of the patients, the lead position was concordant with the maximal delay site. In the responder group, the lateral position was prevalent. The MLHFQ showed a significant improvement in quality of life (p < 0.0002).
Conclusion: CRT determines improvement in the quality of life and in electrical synchronism. Electromechanical synchronism relates to response to CRT. Positioning the LV lead in the maximal delay site has limitations. (Arq Bras Cardiol. 2018; 111(4):607-615)
Keywords: Heart Failure; Cardiac Resynchronization Therapy; Eletrodes,Implanted; Stroke Volume; Radionuclide Imaging.