Volume 110, Nº 4, April 2018
DOI: http://www.dx.doi.org/10.5935/abc.20180038
ORIGINAL ARTICLE
Vimentin and Anti Vimentin Antibodies in Chagas’ Disease
Marilda Savoia Nascimento
Anna Maria Simonsen Stolf
Heitor Franco de Andrade Junior
Ramendra Pati Pandey
Eufrosina Setsu Umezawa
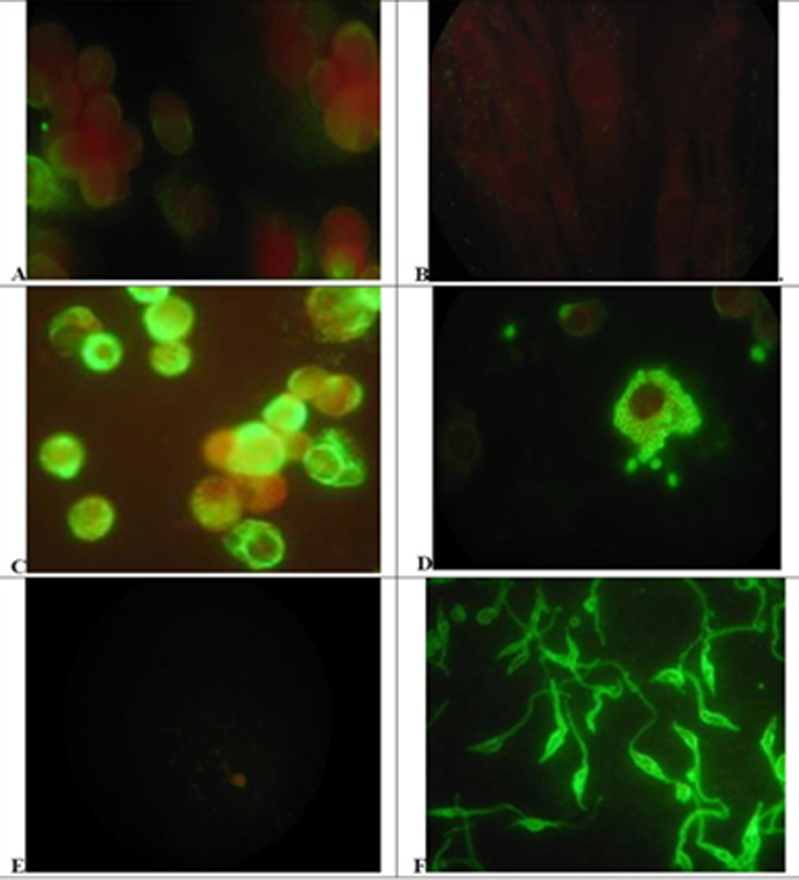
Figure 1 – Distribution of Vimentin or Trypanosoma cruzi antigen on control or infected cells and parasites. A and B) Uninfected LLC MK2 cells reacted to antivimentin abs(A) or anti-T.cruzi abs(B). C and D) T.cruzi infected LLC MK2 cells reacted to antivimentin abs(C) or anti-T.cruzi abs(D). E and F) T.cruzi promastigote forms from in vitro culture reacted to antivimentin abs (E) or anti-T.cruzi abs(F). Cells, infected cells or parasites forms were reacted with Anti Vimentin mAb or chronic infection chagasic serum and revealed with adequate conjugate (x1000) (see Methods).
Abstract
Background: Vimentin is a main structural protein of the cell, a component of intermediate cell filaments and immersed in cytoplasm. Vimentin is mimicked by some bacterial proteins and anti-vimentin antibodies occur in autoimmune cardiac disease, as rheumatic fever. In this work we studied vimentin distribution on LLC-MK2 cells infected with T. cruzi and anti-vimentin antibodies in sera from several clinical pictures of Chagas’ disease or American Trypanosomiasis, in order to elucidate any vimentin involvement in the humoral response of this pathology.
Objective: We standardized an indirect immunofluorescence assay (IFI) to determine sub cellular expression in either parasites and host cells, and ELISA to evaluate anti-vimentin antibodies in sera fron chagasic patients.
Methods: We analyzed the distribution of vimentin in culture cells using indirect fluorescent assays, using as external controls anti-T. cruzi sera, derived from chronic infected patients for identification of the parasites in the same model. After infection and growth of T.cruzi amastigotes, those cells express larger amounts of vimentin, with heavy staining of cytoplasm outside the parasitophorous vacuole and some particle shadowing patterns, suggesting that vimentin are associated with cell cytoplasm. Anti-vimentin antibodies were present in most American trypanosomiasis samples, but notably, they are much more present in acute (76, 9%) or clinical defined syndromes, especially cardiac disease (87, 9%). Paradoxically, they were relatively infrequent in asymptomatic (25%) infected patients, which had a clearly positive serological reaction to parasite antigens, but had low frequency of anti-vimentin antibodies, similar to controls (2,5%).
Conclusion: Our current data revealed that anti-vimentin antibodies induced during T. cruzi infection could be a marker of active disease in the host and its levels could also justify drug therapy in American Trypanosomiasis chronic infection, as a large group of asymptomatic patients would be submitted to treatment with frequent adverse reactions of the available drugs. Anti-vimentin antibodies could be a marker of cardiac muscle cell damage, appearing in American Trypanosomiasis patients during active muscle cell damage. (Arq Bras Cardiol. 2018; 110(4):348-353)
Keywords: Chagas Disease; Heart Diseases; Trypanossoma Cruzi; Rheumatic Fever; Vimentin; Antibodies, Monoclonal.