Volume 110, Nº 2, February 2018
DOI: http://www.dx.doi.org/10.5935/abc.20180018
ORIGINAL ARTICLE
An Alternative Method to Calculate Simplified Projected Aortic Valve Area at Normal Flow Rate
Joana Sofia Silva Moura Ferreira
Nádia Moreira
Rita Ferreira
Sofia Mendes
Rui Martins
Maria João Ferreira
Mariano Pego
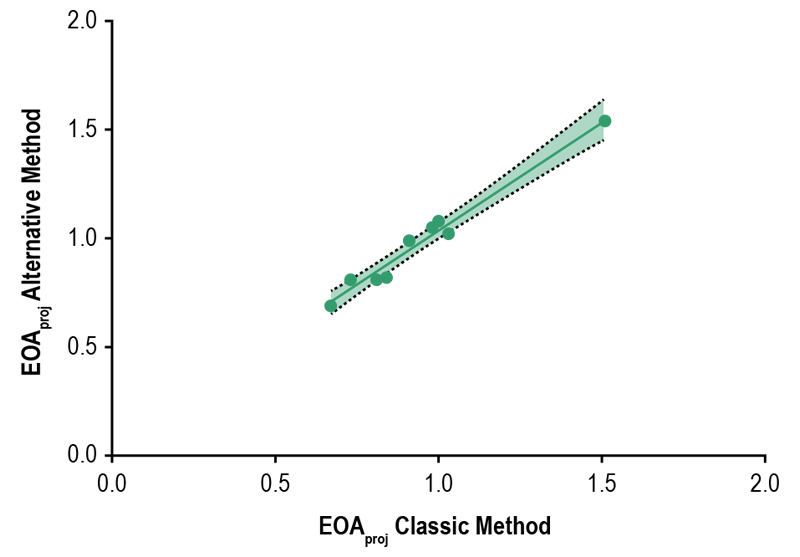
Figure 1 – Scatter plot showing the classic simplified projected aortic valve area values against the alternative simplified projected aortic valve area values with a superimposed regression line (solid line) with 95% confidence bands (dashed lines).
Abstract
Background: Simplified projected aortic valve area (EOAproj) is a valuable echocardiographic parameter in the evaluation of low flow low gradient aortic stenosis (LFLG AS). Its widespread use in clinical practice is hampered by the laborious process of flow rate (Q) calculation.
Objetive: This study proposes a less burdensome, alternative method of Q calculation to be incorporated in the original formula of EOAproj and measures the agreement between the new proposed method of EOAproj calculation and the original one.
Methods: Retrospective observational single-institution study that included all consecutive patients with classic LFLG AS that showed a Q variation with dobutamine infusion ≥ |15|% by both calculation methods.
Results: Twenty-two consecutive patients with classical LFLG AS who underwent dobutamine stress echocardiography were included. Nine patients showed a Q variation with dobutamine infusion calculated by both classical and alternative methods ≥ |15|% and were selected for further statistical analysis. Using the Bland-Altman method to assess agreement we found a systematic bias of 0,037 cm2 (95% CI 0,004 – 0,066), meaning that on average the new method overestimates the EOAproj in 0,037 cm2 compared to the original method. The 95% limits of agreement are narrow (from -0,04 cm2 to 0,12 cm2), meaning that for 95% of individuals, EOAproj calculated by the new method would be between 0,04 cm2 less to 0,12 cm2 more than the EOAproj calculated by the original equation.
Conclusion: The bias and 95% limits of agreement of the new method are narrow and not clinically relevant, supporting the potential interchangeability of the two methods of EOAproj calculation. As the new method requires less additional measurements, it would be easier to implement in clinical practice, promoting an increase in the use of EOAproj. (Arq Bras Cardiol. 2018; 110(2):132-139)
Keywords: Aortic Valve Stenosis / diagnosis; Aortic Valve Stenosis / diagnostic imaging; Echocardiography, Stress; Heart Valves / physiopathology.