Volume 110, Nº 1, January 2018
DOI: http://www.dx.doi.org/10.5935/abc.20170182
ORIGINAL ARTICLE
Sensitive Troponin I Assay in Patients with Chest Pain – Association with Significant Coronary Lesions with or Without Renal Failure
Alexandre de Matos Soeiro
Danielle Menosi Gualandro
Aline Siqueira Bossa
Cindel Nogueira Zullino
Bruno Biselli
Maria Carolina Feres de Almeida Soeiro
Tatiana de Carvalho Andreucci Torres Leal
Carlos Vicente Serrano Jr.
Mucio Tavares de Oliveira Junior
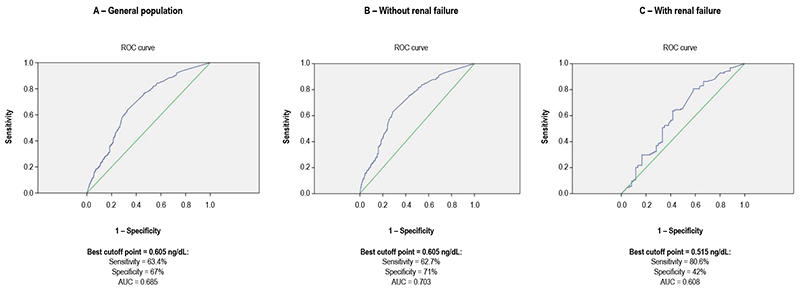
Figure 1 – ROC curve identifying the sensitivity and the specificity of the best cutoff point of troponin as a discriminator of the probability of significant coronary lesion.
AUC: area under the curve.
Abstract
Introduction: Despite having higher sensitivity as compared to conventional troponins, sensitive troponins have lower specificity, mainly in patients with renal failure.
Objective: Study aimed at assessing the sensitive troponin I levels in patients with chest pain, and relating them to the existence of significant coronary lesions.
Methods: Retrospective, single-center, observational. This study included 991 patients divided into two groups: with (N = 681) and without (N = 310) significant coronary lesion. For posterior analysis, the patients were divided into two other groups: with (N = 184) and without (N = 807) chronic renal failure. The commercial ADVIA Centaur® TnI-Ultra assay (Siemens Healthcare Diagnostics) was used. The ROC curve analysis was performed to identify the sensitivity and specificity of the best cutoff point of troponin as a discriminator of the probability of significant coronary lesion. The associations were considered significant when p < 0.05.
Results: The median age was 63 years, and 52% of the patients were of the male sex. The area under the ROC curve between the troponin levels and significant coronary lesions was 0.685 (95% CI: 0.65 – 0.72). In patients with or without renal failure, the areas under the ROC curve were 0.703 (95% CI: 0.66 – 0.74) and 0.608 (95% CI: 0.52 – 0.70), respectively. The best cutoff points to discriminate the presence of significant coronary lesion were: in the general population, 0.605 ng/dL (sensitivity, 63.4%; specificity, 67%); in patients without renal failure, 0.605 ng/dL (sensitivity, 62.7%; specificity, 71%); and in patients with chronic renal failure, 0.515 ng/dL (sensitivity, 80.6%; specificity, 42%).
Conclusion: In patients with chest pain, sensitive troponin I showed a good correlation with significant coronary lesions when its level was greater than 0.605 ng/dL. In patients with chronic renal failure, a significant decrease in specificity was observed in the correlation of troponin levels and severe coronary lesions. (Arq Bras Cardiol. 2018; 110(1):68-73)
Keywords: Troponin I; Chest Pain; Coronary Artery Disease; Renal Insufficiency, Chronic; Biomarkers.